
Medically reviewed for accuracy | Category: Sleep Basics | Reading time: 14 min
It’s 11:47 PM. You have to be up in six and a half hours. You’ve been lying here for forty minutes, perfectly still, eyes closed, doing everything right — and yet your brain has decided that right now is an excellent time to replay an awkward conversation from 2019, recalculate your grocery budget, and wonder whether you left the oven on.
Sound familiar?
If falling asleep feels like something that happens to other people — people who don’t overthink, don’t carry stress home, don’t stare at the ceiling counting shadows — you’re not broken. You’re dealing with something that affects roughly one in three adults. And the good news is that your brain can genuinely be trained to fall asleep faster. Not tricked. Trained.
This guide explains exactly how — grounded in the same science that informs CDC sleep guidelines, written for real people living real lives.
Quick Answer: Key Takeaways
- Falling asleep quickly is a learnable skill, not a personality trait. Your body has natural sleep-onset mechanisms that can be strengthened with consistent habits.
- The CDC recommends at least 7 hours of sleep per night for adults aged 18–60. Consistently taking more than 30 minutes to fall asleep means those 7 hours are starting late every single night.
- Temperature, light, and timing are the three fastest levers for improving sleep onset — more impactful, long-term, than any supplement.
- Trying harder to sleep backfires. Sleep pressure increases the more urgently you chase it. The most effective techniques involve releasing, not forcing.
- Tracking your own patterns is step one. A simple sleep diary — something the CDC itself recommends — reveals the hidden habits that are quietly working against you every night.
- Most cases of difficulty falling asleep are behavioral, not medical. Consistent habit changes over 2–4 weeks produce measurable improvement for the majority of people.
What’s Actually Happening When You Can’t Fall Asleep
Here’s something most people don’t realize: falling asleep isn’t something your brain does passively when you run out of energy. It’s an active biological transition — a carefully orchestrated cascade of events that your nervous system has to initiate deliberately.
For sleep to begin, several things need to happen simultaneously:
Core body temperature must drop. Your body needs to lose about 1–2°F of core heat to trigger sleep onset. This is why a warm bath before bed actually helps you sleep — the subsequent cooling when you step out mimics the temperature drop your brain is waiting for.
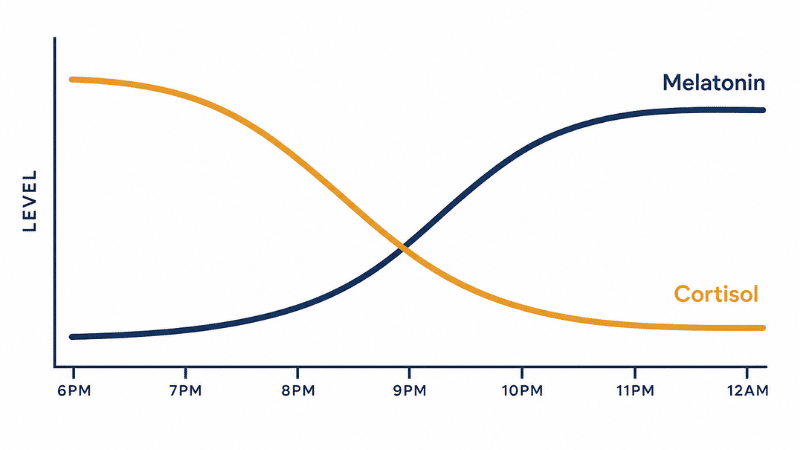
Melatonin must rise. Produced by the pineal gland in response to darkness, melatonin is the biological signal that tells every cell in your body that night has arrived. It doesn’t cause sleep directly — it shifts the nervous system toward its parasympathetic (“rest and digest”) state, creating the conditions for uninterrupted sleep to begin.
Cortisol must fall. Your primary stress and alertness hormone follows a natural daily rhythm: high in the morning to wake you, gradually declining through the day, bottoming out around midnight. When stress, bright light, or irregular sleep schedules keep cortisol elevated into the evening, it actively blocks the sleep-onset process — no matter how tired you feel.
Adenosine pressure must be sufficient. Adenosine is a chemical that accumulates in the brain throughout the day, creating what sleep scientists call “sleep pressure” — the biological drive toward sleep. A sedentary day, a poorly timed nap, or too much caffeine blocking adenosine receptors can leave this pressure lower than your body needs to make sleep easy.
When you lie in bed staring at the ceiling, one or more of these systems is out of sync. Your melatonin is delayed from late-night screen use. Your cortisol is still elevated from stress or alcohol. Your temperature isn’t dropping because the room is too warm. Or your adenosine pressure is lower than it should be because you napped at 5 PM.
There is always a reason sleep won’t come. It is never random, and it is rarely permanent.
What Official Health Guidelines Actually Say
The American Academy of Sleep Medicine (AASM) and the Sleep Research Society define healthy sleep onset latency — the time it takes to fall asleep — as 10 to 20 minutes. Consistently falling asleep in under five minutes is a sign of sleep deprivation, not exceptional sleep talent.
According to the CDC’s official sleep guidelines, the recommended daily sleep duration by age group is:
| Age Group | Recommended Daily Sleep |
|---|---|
| School age (6–12 years) | 9–12 hours |
| Teen (13–17 years) | 8–10 hours |
| Adult (18–60 years) | 7 or more hours |
| Adult (61–64 years) | 7–9 hours |
| Adult (65 years and older) | 7–8 hours |
Yet CDC surveillance data consistently shows that more than one in three American adults regularly fall short of these targets — not always because they don’t have enough time in bed, but because they can’t get to sleep quickly enough, or because their sleep is repeatedly interrupted.
The CDC identifies these as the core signs of poor sleep quality — and they’re worth knowing because many people experience them without connecting them to a solvable problem:
- Trouble falling asleep — taking more than 30 minutes most nights
- Repeatedly waking up during the night — fragmented, non-restorative sleep
- Feeling sleepy or tired even after getting enough hours — a sign the sleep you’re getting isn’t reaching the deeper, restorative stages your body needs
The CDC also recommends specific behavioral habits for better sleep: going to bed and waking at consistent times, keeping the bedroom cool and quiet, avoiding large meals and alcohol before bed, limiting caffeine in the afternoon and evening, and turning off electronic devices at least 30 minutes before bedtime.
These aren’t arbitrary suggestions. They target the exact biological mechanisms — temperature, melatonin, cortisol, adenosine — described above.
The Hidden Cost of Chronic Difficulty Falling Asleep
Most people treat a slow sleep onset as an inconvenience. Understanding the real stakes clarifies why it’s worth actually fixing.
Cognitive performance declines faster than you’d expect. Research from the University of Pennsylvania found that sleeping just 6 hours per night for two weeks produces cognitive deficits equivalent to two full nights of total sleep deprivation — and subjects didn’t feel as impaired as they objectively were. A sleep-deprived brain is a poor judge of its own sleepiness.
The cardiovascular system bears a cumulative cost. The European Heart Journal found that people with chronic insomnia carried a 45% increased risk of heart attack. Disrupted sleep keeps the sympathetic nervous system in a persistently elevated state, driving up blood pressure, systemic inflammation, and long-term cardiovascular strain.
Weight regulation is directly affected. Poor sleep disrupts the balance between ghrelin (the hunger hormone, which rises) and leptin (the satiety signal, which falls). One week of insufficient sleep can increase appetite by up to 24%, with a specific increase in cravings for high-calorie, high-sugar foods — a pattern that builds gradually and imperceptibly.
The immune system is measurably weakened. A landmark study published in Sleep found that people averaging fewer than 7 hours per night were nearly three times more likely to develop a cold when directly exposed to a virus, compared to those sleeping 8 or more hours.
Mental health and sleep are deeply entangled. Anxiety makes falling asleep harder; poor sleep amplifies anxiety. A 2019 study from UC Berkeley found that a single night of insufficient sleep increased anxiety levels by up to 30%. Treating the sleep problem often improves mood and emotional regulation — sometimes more effectively than treating the anxiety directly.
The point is not alarm. The point is context: difficulty falling asleep isn’t a quirk to manage around. It’s a chronic condition with compounding consequences, and it deserves a real solution.
How to Train Your Body to Fall Asleep Faster: 13 Evidence-Based Strategies
Organized from highest to lowest long-term impact, based on current sleep science.
1. Lock In a Fixed Wake Time — Before Anything Else
This is the single most powerful intervention in sleep training, and the most consistently underused. Before you change anything else: pick a wake time and protect it every day, including weekends. Not within an hour — the exact same time.
Your circadian rhythm is anchored primarily by your wake time, not your bedtime. When you rise consistently, your body learns to initiate the sleep-onset process at the right time the night before. Within two to three weeks, many people find themselves growing naturally sleepy at an appropriate hour — not because they forced it, but because their biology recalibrated.
The hardest part: resisting the weekend sleep-in. Extending sleep by 90 minutes on Saturday is the physiological equivalent of flying to a different time zone and back every week — the primary driver of what researchers call “social jet lag,” and the single most common cause of Sunday night insomnia.
2. Use Temperature as a Deliberate Sleep Trigger
Set your bedroom temperature to 65–68°F (18–20°C). This range is consistently identified in sleep research as optimal for sleep onset and deep sleep maintenance — the uninterrupted, restorative stages your body most needs.
If you can’t control room temperature, work with your body directly: a warm bath or shower 60–90 minutes before bed triggers the warming-then-cooling sequence that mimics natural sleep onset. A 2019 meta-analysis in Sleep Medicine Reviews found this reliably reduced sleep onset time by an average of 10 minutes across studies.
Wearing light socks to bed is another practical option — warming the feet accelerates core heat redistribution, and has been shown to speed sleep onset particularly in people who tend to feel cold at night.
3. Manage Light as Carefully as You Manage Caffeine
Light is the primary signal your circadian system uses to set its internal clock — more powerful than most people appreciate.
In the morning: Aim for 10 minutes of natural sunlight within 30 minutes of waking. This anchors your cortisol peak at the appropriate morning hour, which ensures it falls appropriately by evening. On overcast days, a 10,000-lux light therapy lamp is an effective substitute.
In the evening: Begin dimming lights 90 minutes before bed. Blue light from screens suppresses melatonin production by up to 50% — a significant delay in your body’s readiness for sleep. Use blue-light filters on devices, switch to warm-toned lamps, and where possible, put screens down entirely in the final hour before bed. This single change, applied consistently, is one of the fastest ways to shift when your body naturally becomes sleepy.
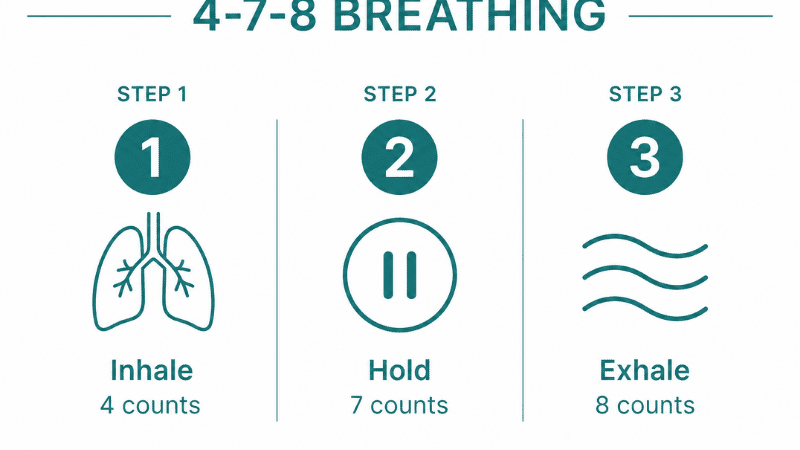
4. Practice 4-7-8 Breathing
Developed by Dr. Andrew Weil and rooted in traditional pranayama breathing, this technique directly activates the parasympathetic nervous system — the physiological state required for sleep onset.
The method:
- Exhale completely through your mouth
- Inhale through your nose for 4 counts
- Hold for 7 counts
- Exhale fully through your mouth for 8 counts
- Repeat for 4 cycles
The extended exhale is the mechanism. Long exhalations stimulate the vagus nerve, which signals the heart to slow and blood pressure to drop. After four cycles, most people notice a genuine physical heaviness — not a forced relaxation, but a real one.
5. Try the Military Sleep Method
Developed to help U.S. military personnel fall asleep in combat conditions, this method is reported to work within two minutes for the majority of people after six weeks of practice.
The sequence:
- Relax your entire face — jaw, tongue, the muscles around your eyes
- Drop your shoulders completely, then relax your upper arms, forearms, and hands
- Exhale and release your chest
- Relax your legs from thighs down to feet
- For 10 seconds, hold a single calm image: lying in a canoe on still water, or resting in a dark hammock. If images don’t come, slowly repeat “don’t think” as a quiet mental anchor.
The key is the sequence — systematic, top-to-bottom physical release paired with deliberate mental emptying.
6. Stop Trying to Fall Asleep (Paradoxical Intention)
This is counterintuitive, but among the most evidence-backed sleep interventions available: paradoxical intention therapy.
Instead of trying to fall asleep, lie still with your eyes open and try — genuinely try — to stay awake. No screens, no reading. Just quiet wakefulness.
This works because sleep effort creates arousal. The more urgently you pursue sleep, the more activated your nervous system becomes, and the further sleep retreats. Removing the performance pressure allows the biological process to proceed naturally. Many people find sleep arrives within minutes of releasing the effort entirely.
7. Reserve the Bed for Sleep Only (Stimulus Control)
This is one of the core components of Cognitive Behavioral Therapy for Insomnia (CBT-I) — the clinical gold standard for sleep difficulty, proven in multiple trials to outperform sleep medication in long-term outcomes.
The principle: the brain learns through association. If you work, scroll, watch, worry, and lie awake in your bed regularly, your brain begins associating your bed with wakefulness. The solution is to use the bed exclusively for sleep — nothing else.
If you’ve been awake for more than 20 minutes, get up. Move to another room, do something calm in dim light, and return only when you feel genuinely sleepy. It feels counterintuitive — almost punishing — but it rapidly rebuilds the bed-sleep association that most poor sleepers have unknowingly eroded over months or years.
8. Time Your Exercise Strategically
Regular physical activity is one of the most powerful long-term interventions for sleep quality. Active people consistently fall asleep faster, spend more time in deep sleep stages, and report better overall sleep quality than sedentary peers.
Timing matters: vigorous exercise raises core temperature and cortisol — ideal in the morning, counterproductive at 9 PM. Finish intense exercise at least three hours before bedtime. Morning and early afternoon exercise produce the strongest sleep benefits.
Gentle movement — yoga, stretching, a slow evening walk — is appropriate any time and actively supports the wind-down process.
9. Cut Caffeine Earlier Than You Think
Caffeine has a half-life of five to seven hours. A 3 PM coffee still has half its stimulant load active at 8–9 PM. For people with slower caffeine metabolism (a genetic variation affecting roughly half the population), the half-life extends to nine or ten hours.
A practical guideline: cut all caffeine sources by 1–2 PM. If you’re a slow metabolizer with persistent sleep difficulty, moving the cutoff to noon for two weeks is a revealing experiment. This applies to tea, pre-workout supplements, energy drinks, and many sodas — not just coffee.
10. Offload Your Mental Agenda Before Bed
Cognitive arousal — the busy, problem-solving, list-running mind — is the most commonly reported barrier to falling asleep. Two techniques address it directly:
The to-do dump: 30–60 minutes before bed (not right at bedtime), write down everything pending for tomorrow — tasks, worries, things you’re afraid of forgetting. Research from Baylor University found that people who completed a written to-do list before bed fell asleep significantly faster than those who wrote about completed tasks. The act of externalizing the mental agenda appears to release the brain from actively holding it.
The cognitive shuffle: Developed by sleep researcher Luc Beaulieu-Prévost, this involves deliberately imagining a random, disconnected sequence of images — a pineapple, a red mailbox, a lighthouse, a foggy path — rather than allowing the mind to follow coherent thought chains. Disjointed imagery mimics the hypnagogic state that naturally precedes sleep and signals the brain to disengage from active processing.
11. Build a Consistent Pre-Sleep Ritual
Your nervous system learns from cues. A consistent sequence of calm behaviors in the 30–60 minutes before bed functions as a biological signal — telling your body that sleep is imminent. Over time, simply beginning the ritual starts to induce drowsiness before you’ve reached the bed.
A simple ritual might include: dimming the lights, brewing a caffeine-free herbal tea (chamomile or spearmint both have documented calming properties), five minutes of light stretching, and 20 minutes of reading a physical book. The specific activities matter less than the consistency. Same order, same time, every night.
12. Consider Magnesium Glycinate
Of all sleep-adjacent supplements, magnesium glycinate has the strongest evidence base for sleep-specific effects. Magnesium plays a direct role in GABA receptor activation — the same pathway targeted by many prescription sleep aids, though far more gently — and supports natural melatonin synthesis.
A significant portion of adults are mildly magnesium-deficient without realizing it. A dose of 200–400mg of magnesium glycinate taken 30–60 minutes before bed is generally well-tolerated. Always consult your healthcare provider if you have kidney conditions or take other medications.
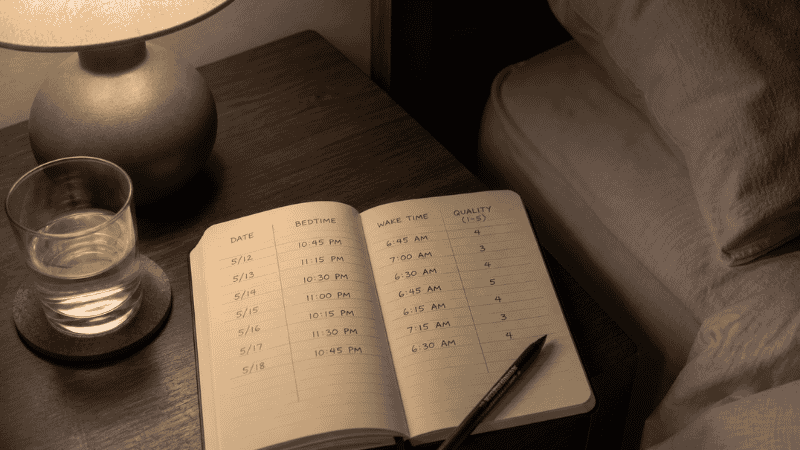
13. Keep a Sleep Diary — The Step Most People Skip
This is the strategy the CDC specifically recommends for people struggling with sleep, and it’s almost universally overlooked in favor of more immediately appealing “fixes.”
A sleep diary doesn’t solve your sleep problem directly. It reveals what’s actually causing it — which is far more valuable than any generic advice, because sleep difficulty is deeply personal. What’s disrupting your sleep is not necessarily what’s disrupting someone else’s.
What to track each day (takes less than 3 minutes):
| Field | What to Record |
|---|---|
| Bedtime | What time you got into bed |
| Time to fall asleep | Estimated minutes before sleep |
| Night wakings | How many times, and approximate duration |
| Wake time | When you actually got up |
| Total sleep | Estimated hours |
| Sleep quality | Simple 1–5 rating |
| Caffeine | Last intake and time |
| Alcohol | Any consumption |
| Exercise | Type, time, and duration |
| Screens | Last use before bed |
| Stress level | Simple 1–5 rating |
| Notes | Anything unusual — travel, illness, late meal |
What to look for after two weeks:
- Do you sleep better on days you exercised?
- Is there a consistent pattern to your worst nights? (Late alcohol? High stress score? Screens after 10 PM?)
- Are you consistently underestimating your time to fall asleep?
- Do you wake at the same time each night? (A specific consistent wake time — say, 3 AM — often points to a specific cause: blood sugar dip, cortisol spike, a noise pattern in your environment.)
The sleep diary transforms vague, chronic sleep difficulty into a solvable, data-driven puzzle. It’s also what a healthcare provider or sleep specialist will ask you to complete before any formal assessment — so keeping one now puts you ahead.
You don’t need an app. A small notebook on your nightstand and 90 seconds of honest observation each morning is enough.
Signs You Should Not Ignore
The strategies above address behavioral sleep difficulty — by far the most common underlying cause. But some symptoms require medical attention rather than habit adjustment.
Talk to a healthcare provider if:
- You consistently take more than 45 minutes to fall asleep even after 4–6 weeks of genuine habit changes
- You or a partner notice you stop breathing during sleep, snore loudly, or gasp awake — these are hallmark signs of sleep apnea, a medical condition requiring specific treatment that behavioral changes alone cannot fix
- You experience an irresistible urge to move your legs at night, often accompanied by uncomfortable crawling or tingling sensations — this describes restless legs syndrome
- You feel overwhelming daytime sleepiness regardless of nightly sleep duration — this may indicate narcolepsy or another sleep disorder
- Your sleep difficulty is accompanied by persistent low mood, loss of interest, or thoughts of self-harm
- You’re relying on alcohol, cannabis, or over-the-counter sleep aids regularly to fall asleep — dependency develops quietly, and these substances disrupt deep sleep architecture in ways that worsen the underlying problem over time
These are not reasons for alarm. They are reasons to get the right kind of help. The CDC notes that healthcare providers can run tests — including formal sleep studies — to identify sleep disorders accurately. Most are highly treatable once properly diagnosed.
Frequently Asked Questions
How long should it normally take to fall asleep? The healthy range is 10–20 minutes. Falling asleep in under 5 minutes suggests significant sleep deprivation. Consistently taking longer than 30 minutes signals that your sleep system needs recalibration.
Why do I fall asleep on the couch but not in bed? This is a textbook sign of conditioned arousal — your brain has associated the bed with wakefulness (from lying awake there repeatedly) and the couch with relaxation. Stimulus control therapy, described in strategy #7, directly addresses this pattern.
Does melatonin actually help you fall asleep faster? Melatonin is most effective for circadian-related sleep difficulty — jet lag, shift work, delayed sleep phase. For general sleep onset issues, its effect is modest. It works better as a timing signal than a sedative. Most over-the-counter doses (3–10mg) are far higher than physiologically necessary; 0.5–1mg is often more effective and better tolerated.
Is it bad to sleep with the TV on? For most people, yes. Even with eyes closed, light from a screen suppresses melatonin and disrupts sleep architecture. Background audio keeps part of the auditory cortex active throughout the night, reducing time in deep sleep stages. If ambient sound helps you sleep, a white noise machine or dedicated sleep sounds device produces a more consistent, non-variable sound environment without the light disruption.
Can anxiety cause a physical inability to sleep? Yes, directly. Anxiety activates the sympathetic nervous system — raising heart rate, elevating cortisol, and producing physiological changes that are fundamentally incompatible with sleep onset. This is one reason treating anxiety often resolves sleep difficulty without directly targeting sleep at all.
What’s a sleep disorder vs. just bad sleep habits? Bad sleep habits respond to behavioral changes within a few weeks. Sleep disorders — insomnia disorder, sleep apnea, restless legs syndrome, narcolepsy — involve physiological mechanisms that behavioral changes alone cannot fully address. The distinction matters for treatment. If consistent habits haven’t moved the needle after 4–6 weeks, a clinical evaluation is the appropriate next step.
How soon will a sleep diary show results? Meaningful patterns typically emerge within 10–14 days of consistent tracking. Two weeks of data gives you and any healthcare provider enough to identify the most likely behavioral drivers of your specific sleep difficulty.
What’s the fastest thing I can do tonight? Cool your room to 65–67°F, do four rounds of 4-7-8 breathing after getting into bed, and if you’re still awake after 20 minutes, get up and sit quietly in dim light until you feel genuinely sleepy. Resisting the urge to lie there “trying harder” is, paradoxically, the fastest path to sleep.
You Can Learn to Fall Asleep — Starting Tonight
The people who sleep well aren’t the ones who found a magic supplement or the perfect mattress. They’re the ones who stopped fighting their bodies and started working with them instead.
Your nervous system wants to sleep. Every biological mechanism you have — melatonin production, adenosine accumulation, the natural evening drop in core temperature and cortisol — is designed to make sleep happen. What’s often standing in the way is a pattern: of late screens, of stress carried into the bedroom, of a bed your brain no longer associates with rest, of habits that were never examined closely enough to be changed.
The sleep diary is where to start. It takes two minutes a morning and two weeks to produce the clearest picture you’ve ever had of what’s actually happening with your sleep. From there, the strategies in this guide give you a structured, evidence-based way to address what you find.
Start with the two highest-leverage changes tonight: set your wake time for tomorrow and cool your bedroom. Add one strategy per week. Track what changes.
Sleep is not a reward for the stress-free. It is a skill — available to anyone willing to build it, patiently and consistently, over time.
You’ve already taken the first step.
Explore more on NourishDAO:
- [Stop Fighting Your Mattress: The Science of Thermal Regulation and Why You Wake Up at 3 AM]
- [Beyond the Pillow: Why Meditation for Sleep Is the Missing Piece of Your Nightly Ritual]
- [Chamomile Tea for Sleep: The Science and Ritual of Nature’s Most Trusted Bedtime Drink]
- [From 40 to 80 ms: How I Doubled My Nightly HRV by Resetting My Circadian Rhythm Protocol]
Sources:
- Centers for Disease Control and Prevention. About Sleep. CDC.gov, May 2024. https://www.cdc.gov/sleep/about/index.html
- American Academy of Sleep Medicine & Sleep Research Society. Recommended Amount of Sleep for a Healthy Adult: A Joint Consensus Statement. Sleep, 2015; 38(6):843–844.
- Haghayegh S, et al. Before-bedtime passive body heating by warm shower or bath to improve sleep. Sleep Medicine Reviews, 2019; 46:124–135.
- Scullin MK, et al. The effects of bedtime writing on difficulty falling asleep. Experimental Brain Research, 2018; 236(6):1–9.
- Simon EB, et al. Overanxious and underslept. Nature Human Behaviour, 2020; 4:100–110.
- Cohen S, et al. Sleep habits and susceptibility to the common cold. Archives of Internal Medicine, 2009; 169(1):62–67.
- Walker M. Why We Sleep: Unlocking the Power of Sleep and Dreams. Scribner, 2017.